29 de mayo 2026
Introduction
Supraventricular tachycardia (SVT) is the most common sustained arrhythmia encountered during pregnancy, and gestational hemodynamic and autonomic changes can increase susceptibility to symptomatic episodes. In hemodynamically stable patients, vagal maneuvers are recommended as first-line therapy, and the REVERT trial showed that the modified Valsalva maneuver was more effective than the standard Valsalva maneuver for acute termination of SVT.
Justification
This case was selected because it highlights a high-yield emergency medicine scenario in which a pregnant patient with stable narrow-complex tachycardia was successfully treated without antiarrhythmic drugs or cardioversion. It is clinically relevant because it illustrates an immediately applicable bedside intervention that may reduce medication exposure during pregnancy while preserving rapid symptom control.
Case description
A 33-year-old pregnant woman at 17 weeks of gestation presented to the emergency department with sudden-onset palpitations and chest tightness after dancing and playing outdoors under sun exposure. Symptoms began abruptly at approximately 12:45 PM, and she denied syncope, severe dyspnea, fever, recent illness, illicit drug use, and known structural heart disease.
Past history and anamnesis
Her relevant past medical history included asthma, with no previously known cardiac disease. The clinical history suggested several potential triggers for the arrhythmic event, including heat exposure, physical exertion, possible mild dehydration, and physiologic cardiovascular changes associated with pregnancy.
Physical examination
On arrival, the patient remained hemodynamically stable despite a regular narrow-complex tachycardia at approximately 214 beats per minute. There were no reported signs of shock, altered mental status, syncope, or severe respiratory distress.
Laboratory and imaging studies
The initial electrocardiogram showed a regular narrow-QRS tachycardia with a ventricular rate of about 214 bpm, regular RR intervals, and no clearly visible P waves, findings compatible with paroxysmal supraventricular tachycardia, most likely atrioventricular nodal reentrant tachycardia. After treatment, a repeat electrocardiogram demonstrated sinus rhythm at approximately 100 bpm, without acute ischemic changes, delta waves, or obvious ventricular pre-excitation.
Laboratory evaluation showed mild hyponatremia with sodium of 134 mmol/L and low-normal potassium of 3.6 mmol/L, while magnesium, calcium, chloride, renal function, and thyroid function remained within acceptable limits. The complete blood count demonstrated mild leukocytosis, mild anemia consistent with pregnancy, and a normal platelet count.
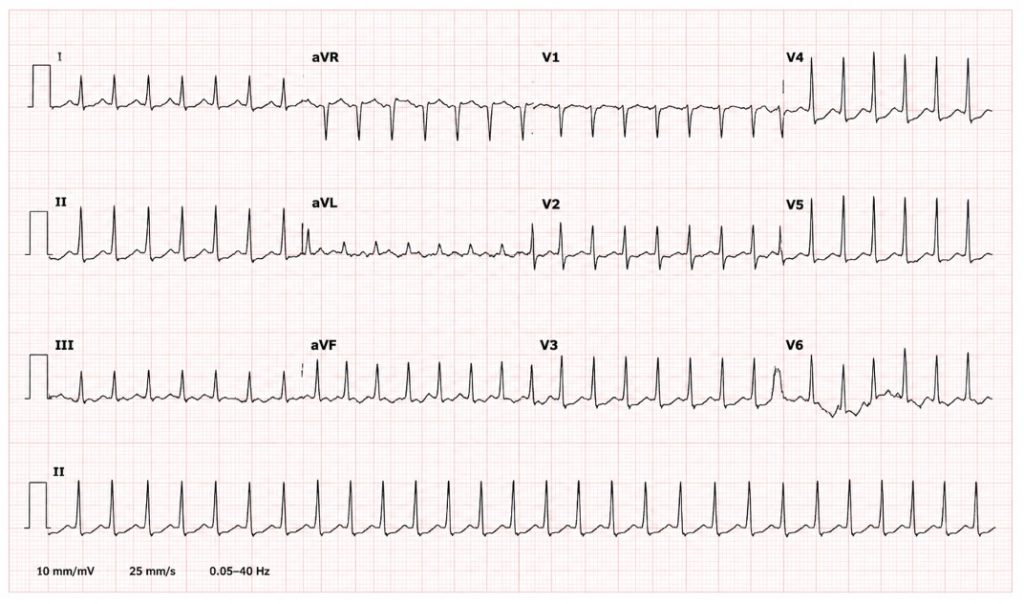
Figura 1. Initial EKG.
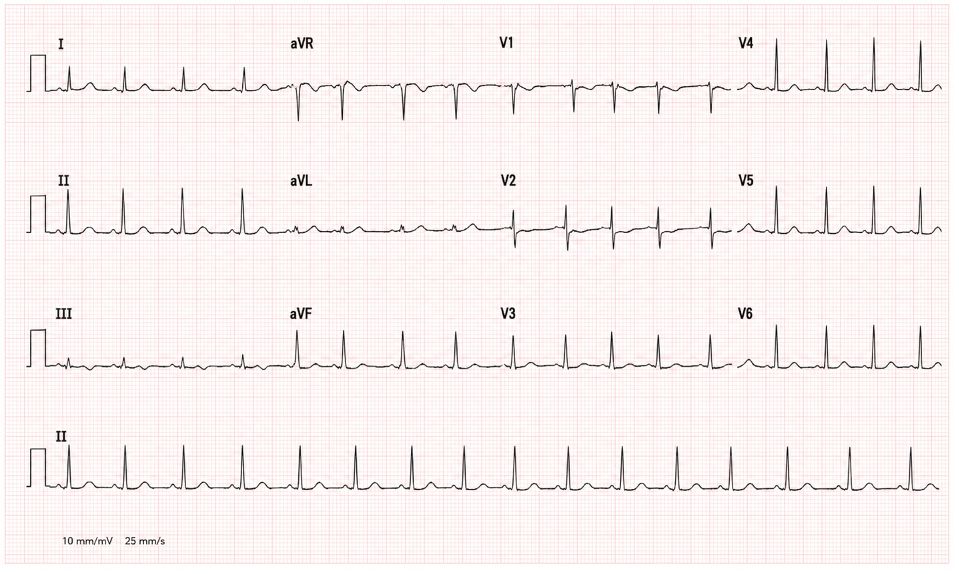
Figura 2. EKG after modified Valsalva maneuver.
Diagnoses
The final diagnosis was paroxysmal supraventricular tachycardia, most likely AVNRT, successfully terminated with the modified Valsalva maneuver. Differential diagnoses included AVRT, atrial tachycardia, and atypical atrial flutter with 1:1 conduction, whereas sinus tachycardia was considered unlikely because of the abrupt onset and high rate.
Expected and obtained results
In a stable patient with regular narrow-complex SVT, the expected immediate goal was rhythm conversion using non-pharmacologic vagal maneuvers before escalation to adenosine. The modified Valsalva maneuver successfully terminated the arrhythmia, restored sinus rhythm, resolved symptoms, and avoided pharmacologic therapy or electrical cardioversion.
Discussion
Pregnancy produces changes in plasma volume, adrenergic tone, and cardiac output that can facilitate supraventricular arrhythmias in susceptible patients. In this case, no major metabolic or structural trigger was identified, making pregnancy-associated physiologic stress, heat exposure, exertion, and probable dehydration the most plausible contributing factors.
The REVERT trial is particularly relevant because it demonstrated a substantially higher cardioversion rate with the modified Valsalva maneuver than with the standard technique in stable SVT, supporting its routine bedside use in emergency care. Current pregnancy-focused reviews also support vagal maneuvers as the initial approach in stable patients and consider adenosine safe when non-pharmacologic treatment fails.
This case reinforces three practical lessons: first, ECG documentation before and after conversion is essential for diagnostic confidence; second, the modified Valsalva maneuver is a fast, low-risk, and medication-sparing strategy; and third, stable SVT during pregnancy can often be managed effectively with structured stepwise emergency care.
References
- Pallas J, O’Neill N, Hill A. Management of gestational supraventricular tachycardia with a ‘modified’ modified Valsalva manoeuvre. Int Emerg Nurs. 2022 Sep;64:101201.
- Appelboam A, Reuben A, Mann C, Gagg J, Ewings P, Barton A, et al. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015 Nov 7;386(10005):1747-53.
- American Heart Association. Adult tachycardia with a pulse algorithm. Dallas: American Heart Association; 2020.
- Managing supraventricular tachyarrhythmia in pregnant patients within the emergency department. Cureus. 2024 Dec 9.
Cite esta colaboración: Héctor Abraham Rojina López “Tachycardia Reverted Without Drugs: Supraventricular Tachycardia at 17 Weeks of Pregnancy Successfully Managed With the Modified Valsalva Maneuver”, blog EMergiendo SMME, mayo 2026. Disponible en: https://emergiendo.org.
Editor revisor: Dr. Manuel Nicanor Caballero Sevilla

Dr. Héctor Abraham Rojina López
-
Emergency Medicine Specialist
-
Family Medical Practice, Ho Chi Minh City, Vietnam
